You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
FATHER QUEST - A Cartoon Network: Villains Victorious CK2-Style Quest Cross Over
- Thread starter HellaCooltricks
- Start date
Threadmarks
View all 40 threadmarks
Reader mode
Reader mode
Recent threadmarks
TURN 7: RESULTS Turn 7: Back To Work 4.21.20XX Interlude: Taking All Callers TURN 6: RIVAL REPORT Interlude: Another Town, Another Monster Interlude: The Truth Stings END Interlude: The Truth Stings (Pt.2) [VOTE] Interlude: The Truth Stings (Pt.1)
Apocrypha
View all 13 threadmarks
Reader mode
Reader mode
Recent threadmarks
Omake: Life of a Candy Pirate: A Sweet Meeting Omake: Giving the Crystal Gems some Shine Omake: I sell (Toilet)Paper and (Toilet)Paper Accessories Omake: Preparing for the Future Omake: Two Fallen Heroes Omakes: Lucky Lydia Makes Some Friends Omake: Tales from the Unknown Vol 1: The Ghost of the Gourds Omake: Hellavator PitchIn my case, neither. Assuming we still need to, we have a Creep to hunt down. Not only will it help the war effort, but it may aid our relations with the Guild (plus, even if it doesn't, forcing Monarch to thank us through gritted teeth will be...Very satisfying). That said, if, for instance, part of the reward for the war council includes giving us that action early...Then, yeah, train Ice Cream Men. We need an actual security force.Well yes ofcourse it will aid our non-combat abillites but not being a raging inferno but rather a controlled and precise flame will aid us in battle quite a bit.
By the way, I would like to check how people are feeling about training our ice creammen vs joining the front once more
I do agree that having The Monarch forced to play nice does sound quite nice (also getting to meet Dr Mrs Monarch would be fun for Father)! I would still like to strike a blow for creating Hardlight factories.In my case, neither. Assuming we still need to, we have a Creep to hunt down. Not only will it help the war effort, but it may aid our relations with the Guild (plus, even if it doesn't, forcing Monarch to thank us through gritted teeth will be...Very satisfying). That said, if, for instance, part of the reward for the war council includes giving us that action early...Then, yeah, train Ice Cream Men. We need an actual security force.
daedalus725
Kell of Kells, godking of Planet X
- Location
- Daedalus crater, The moon
I am for hunting the creep because he might have some cool toys to "liberate"In my case, neither. Assuming we still need to, we have a Creep to hunt down. Not only will it help the war effort, but it may aid our relations with the Guild (plus, even if it doesn't, forcing Monarch to thank us through gritted teeth will be...Very satisfying). That said, if, for instance, part of the reward for the war council includes giving us that action early...Then, yeah, train Ice Cream Men. We need an actual security force.
- Location
- The Golden State
- Pronouns
- He/Him
That is true actually there is two creeps within the city, I am more concern of the racist creep trying to form a gang in our great city of Cleveland, Ohio. We will be doing a great service to the community to rid such threat to make the streets safe for everyoneKeep in mind there are two different Cleveland Creeps running around. Don't pick the wrong one by mistake!
Last edited:
- Location
- USA
I figure Alexis Warrington will handle local villains like that.That is true actually there is two creeps within the city, I am more concern of the racist creep trying to form a gang in our great city of Cleveland, Ohio. We will be doing a great service to the community to rid such threat to make the streets safe for everyone
We need to hunt for Mission Creep, the member of the Peril Partnership which was specifically requested of us by the OSI.
Highly unlikely.Ambivalent, if we take the mass production of the father's shadowsuit we probably could give a boost to the ice cream man that way too.
MrRobot
In doubt there's always the Sun!
It is literally an action we have.
[ ] Synthesise Artificial Shadowstuff (Incompatible with Craft Mantle of The Lesser Dad)
Last edited:
daedalus725
Kell of Kells, godking of Planet X
- Location
- Daedalus crater, The moon
No I believe they mean the ideas that they would be good
MrRobot
In doubt there's always the Sun!
The ice cream man?
Define good.
As a beatstick? Probably not.
As a competent comandos? Deppends how much effort we put into them. Neither training or the artificial shadow suit would be enough on themselves but we have more options than just that
Tadpoleon is one of our qms, so I'm going to believe them when they say no.
I am going to have to disagree with that, they dont need to be the best fighters, all they need is to be good enougth to deal with mook and father can deal with the heavier stuff.The ice cream man?
Define good.
As a beatstick? Probably not.
As a competent comandos? Deppends how much effort we put into them. Neither training or the artificial shadow suit would be enough on themselves but we have more options than just that
TBF, Father can blast through Mooks with the slightest of ease already, man specialises in AoE Fire Attacks.I am going to have to disagree with that, they dont need to be the best fighters, all they need is to be good enougth to deal with mook and father can deal with the heavier stuff.
Artificial Shadowstuff will probably not be applicable to making your ice cream men any better. If you want to use it in a way that will make somebody stronger in a fight, you want the Mantle option.
MrRobot
In doubt there's always the Sun!
It's not that i don't see it but gem tech also works as a building material and KND stuff is very good at going big.
It's not quite appealing when the other option is giving hank a Shadow suit and upgrade his martial description to "He can kick your ass".
It's not quite appealing when the other option is giving hank a Shadow suit and upgrade his martial description to "He can kick your ass".
Last edited:
On Potential Synergistic Interactions of caffeine
- Location
- Pennsylvania
On Potential Synergistic Interactions of caffeine
Abstract
Caffeine is an adenosine A2A receptor antagonist, competitively binding to adenosine receptors in the central nervous system. Antagonism of receptors in the posterior hypothalamus, in conjunction with stimulation of the medullary vagal, vasomotor, and respiratory centers is responsible for the wakefulness-promoting effects. While this is primarily due to the deregulation of adenosine buildup in the neuronal synapse, the increased rate of respiration, decreased heart rate, and vasoconstriction act in the same regard, as does the promotion of the release of monoamines and acetylcholine. Caffeine is metabolized in the liver through the CYP1A2 isozyme resulting in the production of paraxanthine, theobromine, and theophylline, all of which have their own effect on the body. This study investigates potential synergy of other drugs with caffeine to increase the wakefulness-promoting and nootropic effects, as well as other pathways by which CNS stimulation may be achieved, and the downstream effects of adenosine antagonization. Case studies performed will demonstrate that a combination of caffeine with carefully dosed amounts of fluvoxamine and modafinil demonstrate a massive increase in efficacy from all three drugs, making it an ideal choice for commercial applications. Furthermore, earlier stages of the study revealed a combination that is more suited for military use due to the greater effects it has on the body.
Introduction
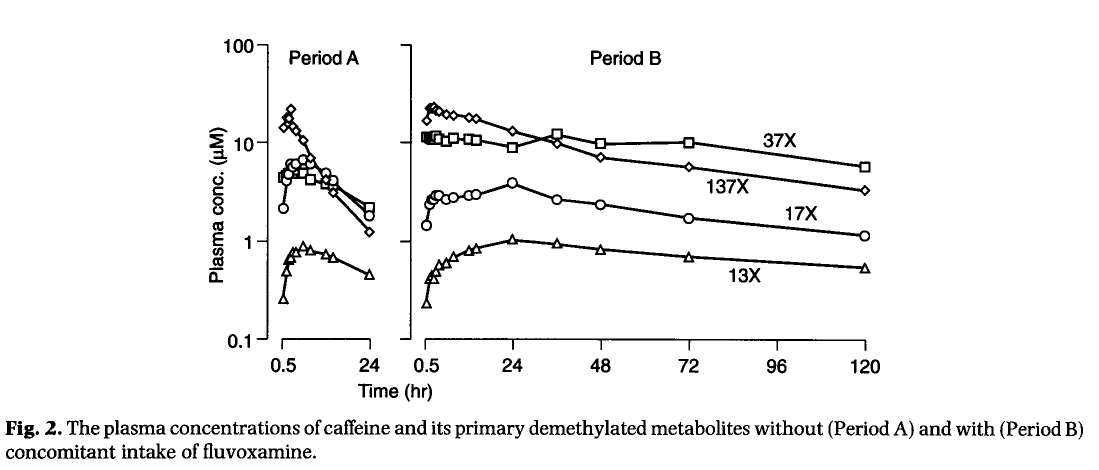
Fluvoxamine is a selective serotonin reuptake inhibitor (SSRI) used primarily for the treatment of major depressive disorder and obsessive-compulsive disorder, functioning by modulating the transport of serotonin into the presynaptic cell via monoamine transporters. With serotonin remaining in the synaptic cleft longer than it normally would, it may act on the synaptic receptors of the recipient cell more than it would have otherwise, playing a role in moderating mood disorders. Fluvoxamine in particular inhibits the function of cytochrome p450 enzyme CYP1A2 which , as the sole mediator in the metabolization of caffeine, increases the bioavailability for up to a 10-fold increase in caffeine levels and subsequent half-life. As seen in U Jeppesen et al, persistent doses of fluvoxamine resulted in consistently elevated caffeine levels present in urine for the aforementioned 10-fold increase. This is statistically significant due to the elimination of caffeine via glomerulal filtration; the majority of caffeine is metabolized in the liver, allowing any remaining in the bloodstream to be excreted- but with CYP1A2 being deactivated by the presence of fluvoxamine, caffeine's plasma concentration is able to remain persistently high. While this does not increase the effect of caffeine on CNS stimulation, it does enhance the duration in which it may act.

As seen above in the experimental protocols dictated by Jeppesen et al, fluvoxamine contributes to the persistence of caffeine and its metabolites for several days following initial consumption, with plasma concentration demonstrating a statistically significant decrease in glomerulal elimination following consumption of fluvoxamine- increasing the half-life from 5 to 31 hours. Jeppesen calls attention to the efficacy of inhibition of CYP1A2 over other substrates such as propranolol, imipramine, and clozapine, eliminating their viability for this project as well as avoiding any potential unwanted side effects of those drugs. Fluvoxamine, therefore, demonstrates viability for use in this indication although further care must be taken to avoid caffeine intoxication.
The mechanism of cocaine is complex and while it has indications involving vasoconstriction and anticoagulant effects, these are unrelated to its potential use in this proposal. Cocaine is a potent CNS simulator, acting primarily on monoamine and reuptake transporters in a similar manner to fluvoxamine- but instead of acting solely on serotonin, cocaine also modulates the concentration of dopamine in the synaptic cleft, leading to the activation of downstream post-synaptic dopamine receptors.Dopaminergic activation of these receptors is involved in the mesolimbic reward pathway that is responsible for habit formation. M Mehta et al examine the synergism of cocaine when administered in conjunction with caffeine, due to their similar yet distinct mechanisms of action in modulating catecholamine release. Caffeine is metabolized primarily in the liver by the cytochrome P450 enzyme, primarily resulting in the release of norepinephrine, while cocaine may act on dopamine and serotonin primarily in preganglionic fibers. (M Mehta et al, 2004) Administration order seems to play a significant role in the demonstrated synergy, due to metabolization rates and affinity for receptors- caffeine may attenuate the effects of cocaine if administered afterwards, but if cocaine is administered following metabolization of caffeine, the synergistic effects may be demonstrated (M Mehta et al, 2004). While this would demonstrate some practical effects in dosing of this combination, the addition of naloxone will decrease the availability of opioid receptors, allowing for the synergy to take place. Naloxone is primarily utilized to counter or reduce the effects of opioid overdose. It is a competitive opioid receptor antagonist, demonstrating a significantly higher binding affinity for the μ-, δ-, and κ-opioid receptors, preventing opioid molecules from continuing their pharmacological effects- and negative side effects such as in the case of respiratory depression (Swerdlow et al, 2005). Oral administration of naloxone results in massively reduced bioavailability compared to intravenous administration due to first-pass metabolism in the liver, resulting in the total amount of available naloxone being insufficient to completely eliminate the effects of the opioid, while still reducing the total amount of opioid metabolization that takes place. This study demonstrates that the presence of naloxone is enough to delay cocaine metabolization after caffeine administration given the half-life of naloxone being shorter than that of cocaine (Handal et al, 1983).
Bubar et al further demonstrate interactions between fluvoxamine and cocaine in mediation of dopamine transmissions in addition to fluvoxamine's effects on serotonin reuptake. Due to the 5-HT serotonin reuptake transporter being modulated by cocaine, this may lead to increased concentrations of serotonin in the synaptic cleft, allowing for SSRIs such as fluvoxamine to potentiate the effects of cocaine (Bubar et al, 2003; Cunningham and Callahan, 1991; Herges and Taylor, 1998; Reith et al., 1991), particularly- and of interest in this study- of the locomotor effects of cocaine. Bubar et al confirms this in their experiment, as was replicated during the experimental phase of this study. It is suggested that this is due to the interaction between 5-HT receptors and their indirect activation by plasma cocaine levels due to fluvoxamine's theorized effect on altering monoamine transporters- " therefore it is plausible that fewer cocaine molecules are able to bind to SERT in the presence of fluoxetine than when cocaine is administered alone, thereby rendering more cocaine available to bind DAT." (Bubar et al, 2003) In essence, this theorizes that the pharmacological activity of cocaine in conjunction with a SSRI like fluvoxamine results in less overall cocaine molecules binding to receptors, thus allowing the effect of cocaine to be modulated by the SSRI, especially in conjunction with the administration of naloxone as previously mentioned. Furthermore, fluvoxamine's inhibition of the P450 3A4 cytochrome (Fleishaker and Hulst, 1994)- the very same mechanism of action by which it synergizes with caffeine- inhibits the breakdown of cocaine, leading to a longer effective half-life of the drug.
The extant possibility of serotonin storm (also known as 'serotonin syndrome') is a possibility with this combination of serotonergic drugs. Serotonin storm is a phenomenon in which synaptic serotonin levels are elevated, causing a wide variety of side effects ranging from an increase in blood pressure to more severe cases such as fever, tremor, and increased sweating (Sternbach 1991). The combination of drugs addressed in this study is unlikely to trigger this phenomenon due to multiple factors as discussed prior- the effects of fluvoxamine and cocaine acting in conjunction, the presence of naloxone decreasing the amount of cocaine binding to opiate receptors- and the lower doses of the SSRI and stimulant, which should reduce the chance to a clinically insignificant 1% of cases (Friedman 2015, Kuribara 1994, Venture et al, 1957). It is unlikely to eliminate the possibility of the phenomenon in its entirety while still utilizing serotonergic drugs, barring the addition of benzodiazepines or serotonin antagonists like cyproheptadine in the case of onset (Friedman 2015). While this would in theory allow us to increase our profits by offering the product ourselves, the risk may be deemed unacceptable for commercial applications despite the lack of risk. There is a noted legal precedent for the lack of liability on companies subcontracted to provide pharmaceuticals to the US Military (United States v. Venture Industries, 1985), leaving this route open to us to pursue. "By providing a black box warning about the appropriate risks of dependence and related symptoms [...] the defendant cannot be held liable for any damages suffered by individual personnel. There is a reasonable degree of competence to be expected in following appropriate dosing directions and management of any resultant side effects." (United States v. Venture Industries, 1985)
This study examines the viability of using armodafinil as an alternative to cocaine in the event that the low risk of serotonin storm is deemed unacceptable for commercial applications. Armodafinil is the R-enantiomer of modafinil, a CNS stimulant that functions on the inhibition of dopamine reuptake. Consequently it has very little effect on the serotonin or norepinephrine receptors (Ishizuka et al, 2012; Schmitt and Reise 2011), instead modulating the effect of the neuropeptide orexin and histamine neurotransmitter pathways, which work in conjunction with dopamine, norepinephrine, and acetylcholine pathways to promote wakefulness as well as stabilizing the need for sleep (Ishizuka et al, 2012). Half-life of the drug is approximately 15 hours in the average Adult body, once again being acted upon by the cytochrome P540 complex (Ninan et al, 2004) providing synergy when administered in conjunction with SSRIs like fluvoxamine due to the ways in which the drugs are metabolized. Most notably, armodafinil's lack of serotonergic activity reduces the possibility of serotonin storm to nonexistent levels when administered in conjunction with caffeine and fluvoxamine (Wisor 2013) given that its only influence on hypothalamic levels of serotonin is the result of a very indirect influence on extracellular dopamine.
Materials and Methods
This study was carried out on a double-blind selection of five hundred Adults who demonstrated no prior heart, liver, or kidney conditions due to clinical investigations, over a period of two months. They consumed no additional drugs nor alcohol over the course of the study, and were subsequently monitored over every step of the procedure, including full panel blood tests, complete urinalysis, EEG, EKG, and physical examination every twenty-four hours. All subjects were told that they were participating in the study but were not informed as to the specifics to avoid any potential placebo contamination.
The following drugs were used: cocaine hydrochloride, fluvoxamine maleate, naloxone hydrochloride, armodafinil, and caffeine. Each was obtained in their purest form from the United States Pharmacopeia, with their purity assured through spectrographic and melting point analysis. Samples were examined and compared to a known baseline and found to be within .05% of the manufacturer's claims, making them suitable for use in the study. All of the drugs were dissolved in sterile 0.9% NaCl saline and administered orally.
The experimental procedures outlined in the study by Jeppesen et al were tested independently to attempt to replicate the results. Subjects were divided randomly into two groups, one of which was monitored on the basis of 200mg caffeine administered over a week, while the experimental group was administered an additional 50mg of fluvoxamine after the first three days, increased to 200mg of fluvoxamine for every subsequent day. Blood plasma and urine samples were collected and analyzed for caffeine metabolites at half hour intervals for the following seventy-two hours. As expected, our own results managed to confirm the protocol dictated by Jeppesen et al, and the experimental protocol could proceed.
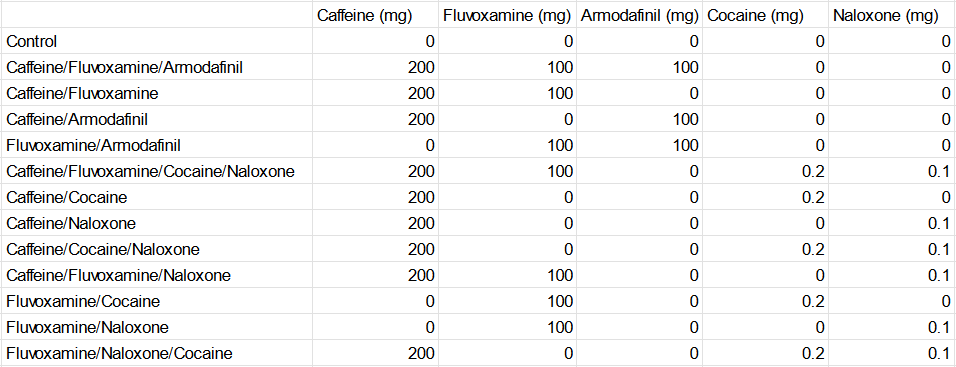
Subsequently, the subjects were randomly divided into thirteen groups, as dictated in the following figure:
Strict monitoring of all subjects was a priority to assure both safety and validity of the data; subjects were provided with food over the course of the protocol that lacked in any potential metabolites of caffeine or the other administered drugs. Over the following two week period, subjects were first administered caffeine for five days prior to concurrent administration of the additional drugs. As mentioned previously, plasma and urine were monitored for metabolites of caffeine, as well as a comprehensive monitoring of heart rate, blood pressure, and coronary flow reserve, as dictated in the following:
[CHARTS REDACTED FOR BREVITY, AVAILABLE ON REQUEST. THERE ARE THREE HUNDRED OF THESE THINGS.]
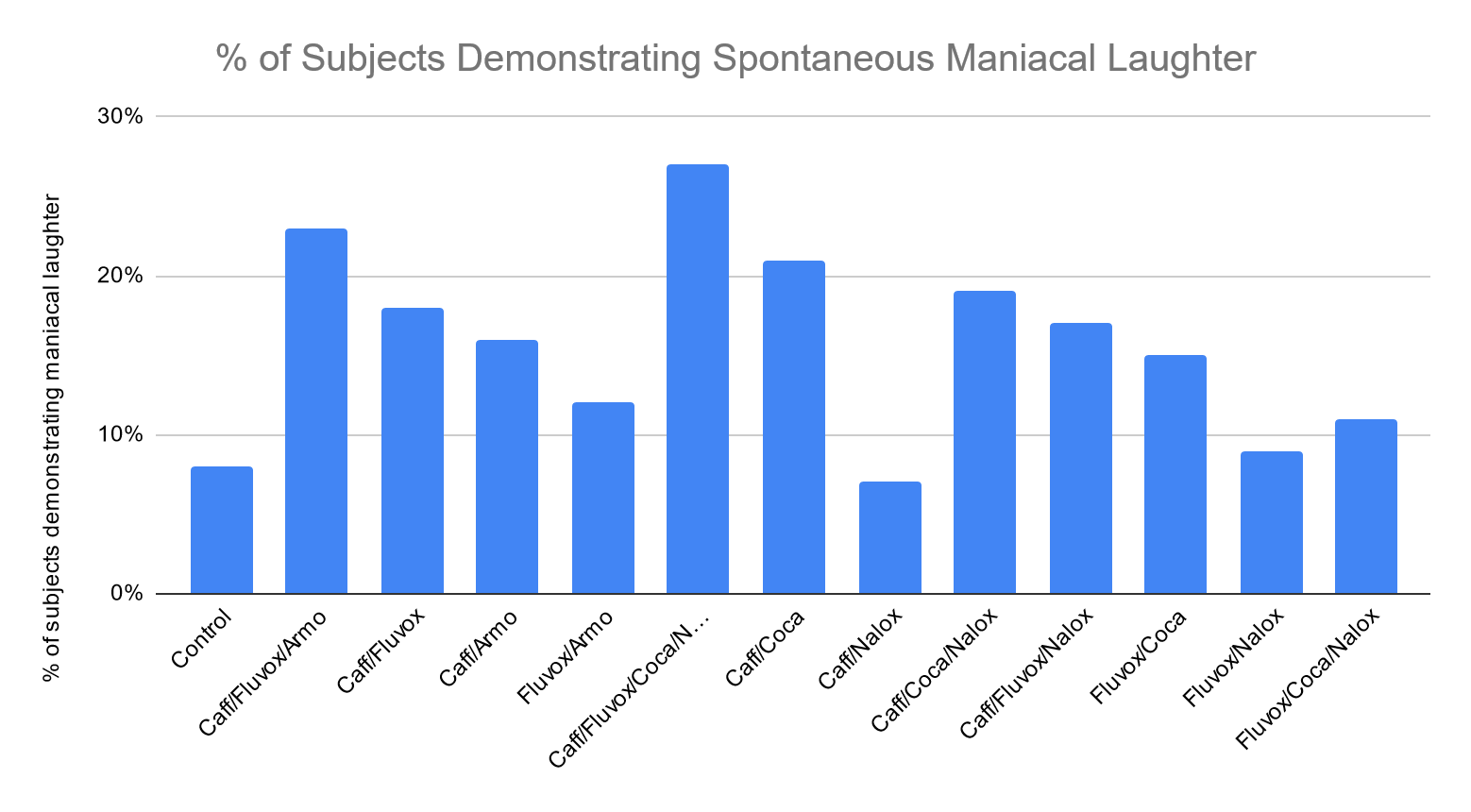
In addition to these physical attributes, the mental effects on test subjects were observed as well, and monitored for any potential deviations from the baseline by means of cognitive tests and interviews. There was a fortunately low occurrence of megalomania within the observed population, with only a grand total of two (2) subjects demonstrating any sort of declaration as to their intent to take on or over the world, while the vast majority of subjects instead displayed increased energy, focus, and efficiency as dictated in the following:
[ANOTHER TWO HUNDRED PAGES OF INTERVIEWS, IT'S REALLY IMPRESSIVE HE DID THIS IN TWO MONTHS]
It should be noted that this study breaks from traditional FDA observation in declaring that spontaneous bouts of laughter, maniacal or otherwise, are a well-observed baseline behavior for many functional Adults. Further study is needed to determine why this behavior tends to increase with administration of different formulations, but at present this is far from a problem.
Discussion
Results of the study are extremely promising. As speculated, the coadministration of caffeine with fluvoxamine, cocaine, and naloxone resulted in suppression of the CYP1A2 enzyme due to fluvoxamine's affinity for the substrate, resulting in vastly increased plasma concentrations of caffeine and subsequently lower concentrations of its metabolites over the drastically increased half-life. Caffeine remained in the blood plasma for up to 31 hours with the expected physiological effects of wakefulness, increased plasma catecholamine concentrations, and other CNS effects. Administration of cocaine hydrochloride in conjunction with a decreased dose of naloxone functioned similar to speculation, with [Figure 31-47] demonstrating the altered locomotor activity, heart rate, blood pressure, myocardial oxygen consumption, and stroke volume as Mehta et al demonstrated. This alone is enough to consider the blend as viable for military applications at the very least, and as expected the occurrence of serotonin storm was extremely low. However, the studies with the combination of caffeine, fluvoxamine, and armodafinil were even more promising [Figures 68-112], in that they demonstrated nootropic effects at the cost of the dramatic change in locomotor activity. These armodafinil studies demonstrated not a single case of dangerously increased serotonin concentration, rendering them perfectly safe for commercial applications. My recommendation in moving into clinical trials is proceeding with two different combinations:
Military application [name pending- investigate 'BATTLE COFFEE' in test markets]: 300 mg caffeine/100 mg fluvoxamine maleate/5 mg cocaine hydrochloride/1 mg naloxone hydrochloride
Civilian application ['Patriarch's TRIFECTA Blend'/'Señor Padre's Café']: 200 mg caffeine/50 mg fluvoxamine maleate/150 mg armodafinil
Obviously, the usual contraindications and dosing considerations apply, though we can absolve ourselves of legal liability by providing a black box warning (Hector con Carne v. FDA, 2023; United States v. Venture Industries, 1957). This product is, of course, for Adults only as its use is strictly contraindicated in any and all children. With the initial trials out of the way, we can move on to more important matters such as finding the perfect blend of coffee to obscure the taste of the pharmaceuticals. I recommend a light blend but will ultimately leave it up to focus groups.
References
Bubar MJ, et al. (2003). "Selective serotonin reuptake inhibitors enhance cocaine-induced locomotor activity and dopamine release in the nucleus accumbens." Neuropharmacology.
Carey RJ, et al. (January 2008). "Cocaine effects on behavioral responding to a novel object placed in a familiar environment". Pharmacology Biochemistry and Behavior.
Fleishaker, J.C., Hulst, L.K., 1994. "A pharmacokinetic and pharmacodynamic evaluation of the combined administration of alprazolam and fluvoxamine." European Journal of Clinical Pharmacology
Friedman, Joseph H. (2015). "Medication-Induced Movement Disorders." Cambridge University Press.
Fujii J, Kuribara H, Tadokoro S. (1989.) "Interaction between caffeine and methamphetamine by means of ambulatory activity in mice. " Yakubutsu Seishin Kodo.
Handal KA, Schauben JL, Salamone FR. (1983) "Naloxone." Ann Emerg Med.
Hector con Carne v. FDA, 771, U.S. 339 (2023)
Ishizuka T, Murotani T, Yamatodani A. (2012) "Action of modafinil through histaminergic and orexinergic neurons." Vitamins and Hormones.
Jeppesen U, et al. (1996). "A fluvoxamine-caffeine interaction study." Pharmacogenetics.
Kuribara H, Uchihashi Y. (1994). "Interactions of opioids with caffeine: evaluation by ambulatory activity in mice." Division for Behavior Analysis, Behavior Research Institute.
Mechner F, Latranyi M. (1963). "Behavioral Effects of Caffeine, Methamphetamine, and Methylphenidate in the Rat." Journal of the Experimental Analysis of Behavior.
Mehta M, et al. (2004). "Effects of cocaine and caffeine alone and in combination on cardiovascular performance." International Journal of Cardiology
Ninan PT, et al. (2004). "Adjunctive modafinil at initiation of treatment with a selective serotonin reuptake inhibitor enhances the degree and onset of therapeutic effects in patients with major depressive disorder and fatigue." Journal of Clinical Psychiatry.
Schmitt KC, Reith ME. (2011) "The atypical stimulant and nootropic modafinil interacts with the dopamine transporter in a different manner than classical cocaine-like inhibitors." PLoS One.
Sternbach H (June 1991). "The serotonin syndrome". American Journal of Psychiatry.
Swerdlow N, et al. (1985). "Effects of Naloxone in Heroin-, Amphetamine-, and Caffeine-Stimulated Locomotor Activity in the Rat." Pharmacology Biochemistry and Behavior.
United States v. Venture Industries, 332, U.S. 214. (1985).
Venture J, et al. (1957). "An Examination into Opiate and Amphetamine Use in Improving US Soldier Efficacy." Journal of Military Ethics.
Wisor J. (2013) "Modafinil as a catecholaminergic agent: empirical evidence and unanswered questions." Frontiers in Neurology.
===
"Huh. Let's see. 'On potential synergistic applications of caffeine'." Hank had been waiting for the Professor's report for what felt like months. He didn't know all that much about chemistry, but as CEO it was going to be his responsibility to figure out just what XXXL had been going on about for all this time and to present it to Mr. Father.
"Hmm. This is a respected scientific journal. I'm sure he doesn't mean that kind of cocaine."
===
"BWAAAH!"
Abstract
Caffeine is an adenosine A2A receptor antagonist, competitively binding to adenosine receptors in the central nervous system. Antagonism of receptors in the posterior hypothalamus, in conjunction with stimulation of the medullary vagal, vasomotor, and respiratory centers is responsible for the wakefulness-promoting effects. While this is primarily due to the deregulation of adenosine buildup in the neuronal synapse, the increased rate of respiration, decreased heart rate, and vasoconstriction act in the same regard, as does the promotion of the release of monoamines and acetylcholine. Caffeine is metabolized in the liver through the CYP1A2 isozyme resulting in the production of paraxanthine, theobromine, and theophylline, all of which have their own effect on the body. This study investigates potential synergy of other drugs with caffeine to increase the wakefulness-promoting and nootropic effects, as well as other pathways by which CNS stimulation may be achieved, and the downstream effects of adenosine antagonization. Case studies performed will demonstrate that a combination of caffeine with carefully dosed amounts of fluvoxamine and modafinil demonstrate a massive increase in efficacy from all three drugs, making it an ideal choice for commercial applications. Furthermore, earlier stages of the study revealed a combination that is more suited for military use due to the greater effects it has on the body.
Introduction
Fluvoxamine is a selective serotonin reuptake inhibitor (SSRI) used primarily for the treatment of major depressive disorder and obsessive-compulsive disorder, functioning by modulating the transport of serotonin into the presynaptic cell via monoamine transporters. With serotonin remaining in the synaptic cleft longer than it normally would, it may act on the synaptic receptors of the recipient cell more than it would have otherwise, playing a role in moderating mood disorders. Fluvoxamine in particular inhibits the function of cytochrome p450 enzyme CYP1A2 which , as the sole mediator in the metabolization of caffeine, increases the bioavailability for up to a 10-fold increase in caffeine levels and subsequent half-life. As seen in U Jeppesen et al, persistent doses of fluvoxamine resulted in consistently elevated caffeine levels present in urine for the aforementioned 10-fold increase. This is statistically significant due to the elimination of caffeine via glomerulal filtration; the majority of caffeine is metabolized in the liver, allowing any remaining in the bloodstream to be excreted- but with CYP1A2 being deactivated by the presence of fluvoxamine, caffeine's plasma concentration is able to remain persistently high. While this does not increase the effect of caffeine on CNS stimulation, it does enhance the duration in which it may act.
As seen above in the experimental protocols dictated by Jeppesen et al, fluvoxamine contributes to the persistence of caffeine and its metabolites for several days following initial consumption, with plasma concentration demonstrating a statistically significant decrease in glomerulal elimination following consumption of fluvoxamine- increasing the half-life from 5 to 31 hours. Jeppesen calls attention to the efficacy of inhibition of CYP1A2 over other substrates such as propranolol, imipramine, and clozapine, eliminating their viability for this project as well as avoiding any potential unwanted side effects of those drugs. Fluvoxamine, therefore, demonstrates viability for use in this indication although further care must be taken to avoid caffeine intoxication.
The mechanism of cocaine is complex and while it has indications involving vasoconstriction and anticoagulant effects, these are unrelated to its potential use in this proposal. Cocaine is a potent CNS simulator, acting primarily on monoamine and reuptake transporters in a similar manner to fluvoxamine- but instead of acting solely on serotonin, cocaine also modulates the concentration of dopamine in the synaptic cleft, leading to the activation of downstream post-synaptic dopamine receptors.Dopaminergic activation of these receptors is involved in the mesolimbic reward pathway that is responsible for habit formation. M Mehta et al examine the synergism of cocaine when administered in conjunction with caffeine, due to their similar yet distinct mechanisms of action in modulating catecholamine release. Caffeine is metabolized primarily in the liver by the cytochrome P450 enzyme, primarily resulting in the release of norepinephrine, while cocaine may act on dopamine and serotonin primarily in preganglionic fibers. (M Mehta et al, 2004) Administration order seems to play a significant role in the demonstrated synergy, due to metabolization rates and affinity for receptors- caffeine may attenuate the effects of cocaine if administered afterwards, but if cocaine is administered following metabolization of caffeine, the synergistic effects may be demonstrated (M Mehta et al, 2004). While this would demonstrate some practical effects in dosing of this combination, the addition of naloxone will decrease the availability of opioid receptors, allowing for the synergy to take place. Naloxone is primarily utilized to counter or reduce the effects of opioid overdose. It is a competitive opioid receptor antagonist, demonstrating a significantly higher binding affinity for the μ-, δ-, and κ-opioid receptors, preventing opioid molecules from continuing their pharmacological effects- and negative side effects such as in the case of respiratory depression (Swerdlow et al, 2005). Oral administration of naloxone results in massively reduced bioavailability compared to intravenous administration due to first-pass metabolism in the liver, resulting in the total amount of available naloxone being insufficient to completely eliminate the effects of the opioid, while still reducing the total amount of opioid metabolization that takes place. This study demonstrates that the presence of naloxone is enough to delay cocaine metabolization after caffeine administration given the half-life of naloxone being shorter than that of cocaine (Handal et al, 1983).
Bubar et al further demonstrate interactions between fluvoxamine and cocaine in mediation of dopamine transmissions in addition to fluvoxamine's effects on serotonin reuptake. Due to the 5-HT serotonin reuptake transporter being modulated by cocaine, this may lead to increased concentrations of serotonin in the synaptic cleft, allowing for SSRIs such as fluvoxamine to potentiate the effects of cocaine (Bubar et al, 2003; Cunningham and Callahan, 1991; Herges and Taylor, 1998; Reith et al., 1991), particularly- and of interest in this study- of the locomotor effects of cocaine. Bubar et al confirms this in their experiment, as was replicated during the experimental phase of this study. It is suggested that this is due to the interaction between 5-HT receptors and their indirect activation by plasma cocaine levels due to fluvoxamine's theorized effect on altering monoamine transporters- " therefore it is plausible that fewer cocaine molecules are able to bind to SERT in the presence of fluoxetine than when cocaine is administered alone, thereby rendering more cocaine available to bind DAT." (Bubar et al, 2003) In essence, this theorizes that the pharmacological activity of cocaine in conjunction with a SSRI like fluvoxamine results in less overall cocaine molecules binding to receptors, thus allowing the effect of cocaine to be modulated by the SSRI, especially in conjunction with the administration of naloxone as previously mentioned. Furthermore, fluvoxamine's inhibition of the P450 3A4 cytochrome (Fleishaker and Hulst, 1994)- the very same mechanism of action by which it synergizes with caffeine- inhibits the breakdown of cocaine, leading to a longer effective half-life of the drug.
The extant possibility of serotonin storm (also known as 'serotonin syndrome') is a possibility with this combination of serotonergic drugs. Serotonin storm is a phenomenon in which synaptic serotonin levels are elevated, causing a wide variety of side effects ranging from an increase in blood pressure to more severe cases such as fever, tremor, and increased sweating (Sternbach 1991). The combination of drugs addressed in this study is unlikely to trigger this phenomenon due to multiple factors as discussed prior- the effects of fluvoxamine and cocaine acting in conjunction, the presence of naloxone decreasing the amount of cocaine binding to opiate receptors- and the lower doses of the SSRI and stimulant, which should reduce the chance to a clinically insignificant 1% of cases (Friedman 2015, Kuribara 1994, Venture et al, 1957). It is unlikely to eliminate the possibility of the phenomenon in its entirety while still utilizing serotonergic drugs, barring the addition of benzodiazepines or serotonin antagonists like cyproheptadine in the case of onset (Friedman 2015). While this would in theory allow us to increase our profits by offering the product ourselves, the risk may be deemed unacceptable for commercial applications despite the lack of risk. There is a noted legal precedent for the lack of liability on companies subcontracted to provide pharmaceuticals to the US Military (United States v. Venture Industries, 1985), leaving this route open to us to pursue. "By providing a black box warning about the appropriate risks of dependence and related symptoms [...] the defendant cannot be held liable for any damages suffered by individual personnel. There is a reasonable degree of competence to be expected in following appropriate dosing directions and management of any resultant side effects." (United States v. Venture Industries, 1985)
This study examines the viability of using armodafinil as an alternative to cocaine in the event that the low risk of serotonin storm is deemed unacceptable for commercial applications. Armodafinil is the R-enantiomer of modafinil, a CNS stimulant that functions on the inhibition of dopamine reuptake. Consequently it has very little effect on the serotonin or norepinephrine receptors (Ishizuka et al, 2012; Schmitt and Reise 2011), instead modulating the effect of the neuropeptide orexin and histamine neurotransmitter pathways, which work in conjunction with dopamine, norepinephrine, and acetylcholine pathways to promote wakefulness as well as stabilizing the need for sleep (Ishizuka et al, 2012). Half-life of the drug is approximately 15 hours in the average Adult body, once again being acted upon by the cytochrome P540 complex (Ninan et al, 2004) providing synergy when administered in conjunction with SSRIs like fluvoxamine due to the ways in which the drugs are metabolized. Most notably, armodafinil's lack of serotonergic activity reduces the possibility of serotonin storm to nonexistent levels when administered in conjunction with caffeine and fluvoxamine (Wisor 2013) given that its only influence on hypothalamic levels of serotonin is the result of a very indirect influence on extracellular dopamine.
Materials and Methods
This study was carried out on a double-blind selection of five hundred Adults who demonstrated no prior heart, liver, or kidney conditions due to clinical investigations, over a period of two months. They consumed no additional drugs nor alcohol over the course of the study, and were subsequently monitored over every step of the procedure, including full panel blood tests, complete urinalysis, EEG, EKG, and physical examination every twenty-four hours. All subjects were told that they were participating in the study but were not informed as to the specifics to avoid any potential placebo contamination.
The following drugs were used: cocaine hydrochloride, fluvoxamine maleate, naloxone hydrochloride, armodafinil, and caffeine. Each was obtained in their purest form from the United States Pharmacopeia, with their purity assured through spectrographic and melting point analysis. Samples were examined and compared to a known baseline and found to be within .05% of the manufacturer's claims, making them suitable for use in the study. All of the drugs were dissolved in sterile 0.9% NaCl saline and administered orally.
The experimental procedures outlined in the study by Jeppesen et al were tested independently to attempt to replicate the results. Subjects were divided randomly into two groups, one of which was monitored on the basis of 200mg caffeine administered over a week, while the experimental group was administered an additional 50mg of fluvoxamine after the first three days, increased to 200mg of fluvoxamine for every subsequent day. Blood plasma and urine samples were collected and analyzed for caffeine metabolites at half hour intervals for the following seventy-two hours. As expected, our own results managed to confirm the protocol dictated by Jeppesen et al, and the experimental protocol could proceed.
Subsequently, the subjects were randomly divided into thirteen groups, as dictated in the following figure:
Strict monitoring of all subjects was a priority to assure both safety and validity of the data; subjects were provided with food over the course of the protocol that lacked in any potential metabolites of caffeine or the other administered drugs. Over the following two week period, subjects were first administered caffeine for five days prior to concurrent administration of the additional drugs. As mentioned previously, plasma and urine were monitored for metabolites of caffeine, as well as a comprehensive monitoring of heart rate, blood pressure, and coronary flow reserve, as dictated in the following:
[CHARTS REDACTED FOR BREVITY, AVAILABLE ON REQUEST. THERE ARE THREE HUNDRED OF THESE THINGS.]
In addition to these physical attributes, the mental effects on test subjects were observed as well, and monitored for any potential deviations from the baseline by means of cognitive tests and interviews. There was a fortunately low occurrence of megalomania within the observed population, with only a grand total of two (2) subjects demonstrating any sort of declaration as to their intent to take on or over the world, while the vast majority of subjects instead displayed increased energy, focus, and efficiency as dictated in the following:
[ANOTHER TWO HUNDRED PAGES OF INTERVIEWS, IT'S REALLY IMPRESSIVE HE DID THIS IN TWO MONTHS]
It should be noted that this study breaks from traditional FDA observation in declaring that spontaneous bouts of laughter, maniacal or otherwise, are a well-observed baseline behavior for many functional Adults. Further study is needed to determine why this behavior tends to increase with administration of different formulations, but at present this is far from a problem.
Discussion
Results of the study are extremely promising. As speculated, the coadministration of caffeine with fluvoxamine, cocaine, and naloxone resulted in suppression of the CYP1A2 enzyme due to fluvoxamine's affinity for the substrate, resulting in vastly increased plasma concentrations of caffeine and subsequently lower concentrations of its metabolites over the drastically increased half-life. Caffeine remained in the blood plasma for up to 31 hours with the expected physiological effects of wakefulness, increased plasma catecholamine concentrations, and other CNS effects. Administration of cocaine hydrochloride in conjunction with a decreased dose of naloxone functioned similar to speculation, with [Figure 31-47] demonstrating the altered locomotor activity, heart rate, blood pressure, myocardial oxygen consumption, and stroke volume as Mehta et al demonstrated. This alone is enough to consider the blend as viable for military applications at the very least, and as expected the occurrence of serotonin storm was extremely low. However, the studies with the combination of caffeine, fluvoxamine, and armodafinil were even more promising [Figures 68-112], in that they demonstrated nootropic effects at the cost of the dramatic change in locomotor activity. These armodafinil studies demonstrated not a single case of dangerously increased serotonin concentration, rendering them perfectly safe for commercial applications. My recommendation in moving into clinical trials is proceeding with two different combinations:
Military application [name pending- investigate 'BATTLE COFFEE' in test markets]: 300 mg caffeine/100 mg fluvoxamine maleate/5 mg cocaine hydrochloride/1 mg naloxone hydrochloride
Civilian application ['Patriarch's TRIFECTA Blend'/'Señor Padre's Café']: 200 mg caffeine/50 mg fluvoxamine maleate/150 mg armodafinil
Obviously, the usual contraindications and dosing considerations apply, though we can absolve ourselves of legal liability by providing a black box warning (Hector con Carne v. FDA, 2023; United States v. Venture Industries, 1957). This product is, of course, for Adults only as its use is strictly contraindicated in any and all children. With the initial trials out of the way, we can move on to more important matters such as finding the perfect blend of coffee to obscure the taste of the pharmaceuticals. I recommend a light blend but will ultimately leave it up to focus groups.
References
Bubar MJ, et al. (2003). "Selective serotonin reuptake inhibitors enhance cocaine-induced locomotor activity and dopamine release in the nucleus accumbens." Neuropharmacology.
Carey RJ, et al. (January 2008). "Cocaine effects on behavioral responding to a novel object placed in a familiar environment". Pharmacology Biochemistry and Behavior.
Fleishaker, J.C., Hulst, L.K., 1994. "A pharmacokinetic and pharmacodynamic evaluation of the combined administration of alprazolam and fluvoxamine." European Journal of Clinical Pharmacology
Friedman, Joseph H. (2015). "Medication-Induced Movement Disorders." Cambridge University Press.
Fujii J, Kuribara H, Tadokoro S. (1989.) "Interaction between caffeine and methamphetamine by means of ambulatory activity in mice. " Yakubutsu Seishin Kodo.
Handal KA, Schauben JL, Salamone FR. (1983) "Naloxone." Ann Emerg Med.
Hector con Carne v. FDA, 771, U.S. 339 (2023)
Ishizuka T, Murotani T, Yamatodani A. (2012) "Action of modafinil through histaminergic and orexinergic neurons." Vitamins and Hormones.
Jeppesen U, et al. (1996). "A fluvoxamine-caffeine interaction study." Pharmacogenetics.
Kuribara H, Uchihashi Y. (1994). "Interactions of opioids with caffeine: evaluation by ambulatory activity in mice." Division for Behavior Analysis, Behavior Research Institute.
Mechner F, Latranyi M. (1963). "Behavioral Effects of Caffeine, Methamphetamine, and Methylphenidate in the Rat." Journal of the Experimental Analysis of Behavior.
Mehta M, et al. (2004). "Effects of cocaine and caffeine alone and in combination on cardiovascular performance." International Journal of Cardiology
Ninan PT, et al. (2004). "Adjunctive modafinil at initiation of treatment with a selective serotonin reuptake inhibitor enhances the degree and onset of therapeutic effects in patients with major depressive disorder and fatigue." Journal of Clinical Psychiatry.
Schmitt KC, Reith ME. (2011) "The atypical stimulant and nootropic modafinil interacts with the dopamine transporter in a different manner than classical cocaine-like inhibitors." PLoS One.
Sternbach H (June 1991). "The serotonin syndrome". American Journal of Psychiatry.
Swerdlow N, et al. (1985). "Effects of Naloxone in Heroin-, Amphetamine-, and Caffeine-Stimulated Locomotor Activity in the Rat." Pharmacology Biochemistry and Behavior.
United States v. Venture Industries, 332, U.S. 214. (1985).
Venture J, et al. (1957). "An Examination into Opiate and Amphetamine Use in Improving US Soldier Efficacy." Journal of Military Ethics.
Wisor J. (2013) "Modafinil as a catecholaminergic agent: empirical evidence and unanswered questions." Frontiers in Neurology.
===
"Huh. Let's see. 'On potential synergistic applications of caffeine'." Hank had been waiting for the Professor's report for what felt like months. He didn't know all that much about chemistry, but as CEO it was going to be his responsibility to figure out just what XXXL had been going on about for all this time and to present it to Mr. Father.
"Hmm. This is a respected scientific journal. I'm sure he doesn't mean that kind of cocaine."
===
"BWAAAH!"
MrRobot
In doubt there's always the Sun!
Knowing XXXL is not that kind of coaine but rather a super voaine with no negative effect he made fo fun. He sure as hell will not be able to explain it trough.Hmm. This is a respected scientific journal. I'm sure he doesn't mean that kind of cocaine."
- Location
- USA
You might think that...Knowing XXXL is not that kind of coaine but rather a super voaine with no negative effect he made fo fun. He sure as hell will not be able to explain it trough.
Threadmarks
View all 40 threadmarks
Reader mode
Reader mode
Recent threadmarks
TURN 7: RESULTS Turn 7: Back To Work 4.21.20XX Interlude: Taking All Callers TURN 6: RIVAL REPORT Interlude: Another Town, Another Monster Interlude: The Truth Stings END Interlude: The Truth Stings (Pt.2) [VOTE] Interlude: The Truth Stings (Pt.1)
Apocrypha
View all 13 threadmarks
Reader mode
Reader mode